-
×
 Medical hygroscopic surgical absorbent cotton Variant non-sterile, 250 g 1 pc
1 × €6.26
Medical hygroscopic surgical absorbent cotton Variant non-sterile, 250 g 1 pc
1 × €6.26 -
×
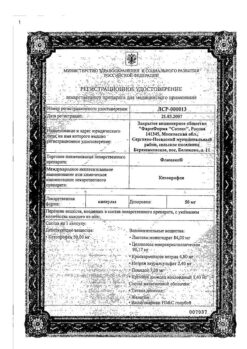
Solgar Coenzyme Q10, 60 mg capsules 30 pcs.
1 × €46.54
-
×
Terbinafin, cream 1% 30 g
1 × €8.78
-
×
Martens rubber bandage 5 m, 1 pc
1 × €16.71
-
×
 Singular, 5 mg 14 pcs
1 × €31.41
Singular, 5 mg 14 pcs
1 × €31.41 -
×
First Aid Pantenol children's spray Wounds A Burns, 130 g
1 × €8.12
-
×
🐾 ZooVip Joint Cream Balm Glucosamine + Chondraotin, 500 ml
1 × €11.58
-
×
🐾 ZooVip Relaxing Gel with Peppermint and Lavender, 500 ml
1 × €10.87
-
×
Stresam, 50 mg capsules 60 pcs
1 × €47.05
-
×
Arthro-Aktiv warming balm, 20 g
1 × €6.74
 Medical hygroscopic surgical absorbent cotton Variant non-sterile, 250 g 1 pc
Medical hygroscopic surgical absorbent cotton Variant non-sterile, 250 g 1 pc  Solgar Coenzyme Q10, 60 mg capsules 30 pcs.
Solgar Coenzyme Q10, 60 mg capsules 30 pcs.  Terbinafin, cream 1% 30 g
Terbinafin, cream 1% 30 g  Martens rubber bandage 5 m, 1 pc
Martens rubber bandage 5 m, 1 pc  Singular, 5 mg 14 pcs
Singular, 5 mg 14 pcs  First Aid Pantenol children's spray Wounds A Burns, 130 g
First Aid Pantenol children's spray Wounds A Burns, 130 g  🐾 ZooVip Joint Cream Balm Glucosamine + Chondraotin, 500 ml
🐾 ZooVip Joint Cream Balm Glucosamine + Chondraotin, 500 ml  🐾 ZooVip Relaxing Gel with Peppermint and Lavender, 500 ml
🐾 ZooVip Relaxing Gel with Peppermint and Lavender, 500 ml  Stresam, 50 mg capsules 60 pcs
Stresam, 50 mg capsules 60 pcs  Arthro-Aktiv warming balm, 20 g
Arthro-Aktiv warming balm, 20 g Subtotal: €194.06