-
×
 Phenystil, drops 1 mg/ml 20 ml
1 × €14.43
Phenystil, drops 1 mg/ml 20 ml
1 × €14.43 -
×
Vizmed multi, 0.18% 10 ml
1 × €18.84
-
×
🐾 Beaphar Stop It Cat Repellent Spray for cats, 100 ml
1 × €21.56
-
×
Satellite Express test strips, 50 pcs.
1 × €13.52
-
×
Herbal tea Altai #6 soothing, filter packs, 20 pcs.
1 × €5.61
-
×
Polyvalent piobacteriophage, 20 ml 4 pcs
1 × €23.45
-
×
Lotonel, tablets 5 mg 60 pcs
1 × €14.32
-
×
Atheroklefit Bio, capsules, 30 pcs.
1 × €11.10
-
×
Pancragen, capsules 0.2 g, 60 pcs.
1 × €21.44
-
×
Artro-Aktiv capsules, 36 pcs.
1 × €6.31
 Phenystil, drops 1 mg/ml 20 ml
Phenystil, drops 1 mg/ml 20 ml  Vizmed multi, 0.18% 10 ml
Vizmed multi, 0.18% 10 ml 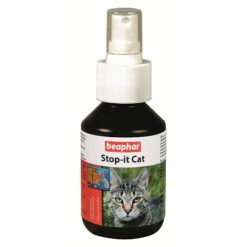 🐾 Beaphar Stop It Cat Repellent Spray for cats, 100 ml
🐾 Beaphar Stop It Cat Repellent Spray for cats, 100 ml  Satellite Express test strips, 50 pcs.
Satellite Express test strips, 50 pcs.  Herbal tea Altai #6 soothing, filter packs, 20 pcs.
Herbal tea Altai #6 soothing, filter packs, 20 pcs.  Polyvalent piobacteriophage, 20 ml 4 pcs
Polyvalent piobacteriophage, 20 ml 4 pcs  Lotonel, tablets 5 mg 60 pcs
Lotonel, tablets 5 mg 60 pcs  Atheroklefit Bio, capsules, 30 pcs.
Atheroklefit Bio, capsules, 30 pcs.  Pancragen, capsules 0.2 g, 60 pcs.
Pancragen, capsules 0.2 g, 60 pcs.  Artro-Aktiv capsules, 36 pcs.
Artro-Aktiv capsules, 36 pcs. Subtotal: €150.58