-
×
 Formetin, tablets 500 mg 60 pcs
1 × €3.24
Formetin, tablets 500 mg 60 pcs
1 × €3.24 -
×
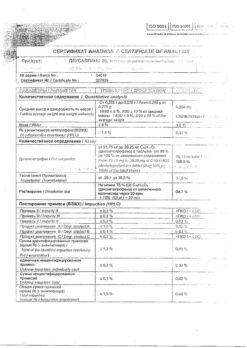
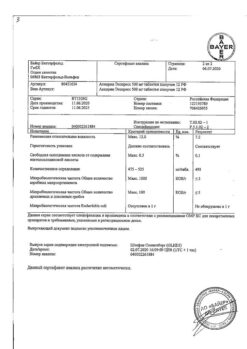
 Duodart, 0.5 mg+0.4 mg 90 pcs
1 × €114.61
Duodart, 0.5 mg+0.4 mg 90 pcs
1 × €114.61 -
×
Vitamin C tablets effervescent 1200 mg 10 pcs.
1 × €6.19
-
×
Suglat, 50 mg 30 pcs
1 × €57.72
-
×
OneTouch Select Plus Test Strips, 50 pcs.
1 × €27.30
-
×
Herbal tea Altai № 21 pankrefit, filter packs, 20 pcs.
1 × €5.19
-
×
Inoltra, capsules, 180 pcs.
1 × €232.09
-
×
Arthro-Aktiv warming balm, 20 g
1 × €6.74
-
×
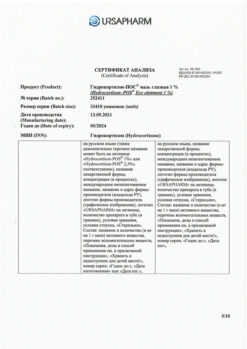
Chlorhexidine, 0.05% solution 100 ml
1 × €0.44
-
×
Suprenamine 155 mg, enteric-soluble tablets 40 pcs
1 × €15.69
 Formetin, tablets 500 mg 60 pcs
Formetin, tablets 500 mg 60 pcs  Duodart, 0.5 mg+0.4 mg 90 pcs
Duodart, 0.5 mg+0.4 mg 90 pcs  Vitamin C tablets effervescent 1200 mg 10 pcs.
Vitamin C tablets effervescent 1200 mg 10 pcs.  Suglat, 50 mg 30 pcs
Suglat, 50 mg 30 pcs  OneTouch Select Plus Test Strips, 50 pcs.
OneTouch Select Plus Test Strips, 50 pcs.  Herbal tea Altai № 21 pankrefit, filter packs, 20 pcs.
Herbal tea Altai № 21 pankrefit, filter packs, 20 pcs.  Inoltra, capsules, 180 pcs.
Inoltra, capsules, 180 pcs.  Arthro-Aktiv warming balm, 20 g
Arthro-Aktiv warming balm, 20 g  Chlorhexidine, 0.05% solution 100 ml
Chlorhexidine, 0.05% solution 100 ml  Suprenamine 155 mg, enteric-soluble tablets 40 pcs
Suprenamine 155 mg, enteric-soluble tablets 40 pcs Subtotal: €469.21