-
×
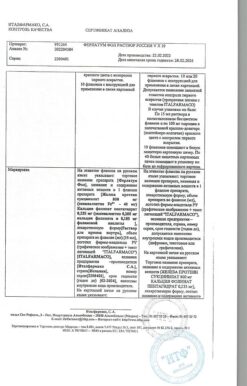
 Ferrum Lek, 50 mg/ml 2 ml 50 pcs
1 × €202.54
Ferrum Lek, 50 mg/ml 2 ml 50 pcs
1 × €202.54 -
×
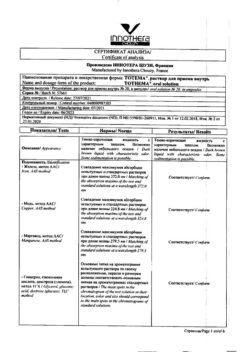
Totema, 10 ml 20 pcs.
1 × €14.39
Subtotal: €216.93
 Ferrum Lek, 50 mg/ml 2 ml 50 pcs
1 × €202.54
Ferrum Lek, 50 mg/ml 2 ml 50 pcs
1 × €202.54 Totema, 10 ml 20 pcs.
1 × €14.39
Totema, 10 ml 20 pcs.
1 × €14.39Subtotal: €216.93

€1.00
Out of stock
Pharmacotherapeutic group: iron drug.
The ATX code: B03AE10
Pharmacological action
.Pharmacodynamics
Iron is the body’s most important micronutrient. As a coenzyme of cytochrome oxidase, catalase and peroxidase, as well as a component of hemoglobin (Hb), myoglobin and cytochromes, it is involved in many metabolic processes and stimulates erythropoiesis.
The serine α-amino acid contained in the drug promotes more effective absorption of iron and its entry into the systemic bloodstream, resulting in rapid recovery of its normal content in the body. This provides better tolerability of the drug and reduces the amount of iron required.
The daily requirement for iron in adults is 1-2 mg, in pregnant women 2-5 mg, in children under 7 years of age 0.5-1.5 mg. On average, 10% is absorbed, so in order to meet the need for iron, the dose when taken orally must be 10 times the daily requirement.
Pharmacokinetics
After oral administration, about 10-15% of divalent iron is absorbed in the duodenum and jejunum. Absorption of iron is also possible through the mechanism of passive diffusion. Absorption of iron is significantly increased in iron deficiency and in increased erythropoiesis. In patients with low hemoglobin and depleted iron depot, absorption may increase up to 50-60% and decrease with normalization of these parameters. The maximum concentration of iron is reached 2-4 hours after intake.
In the blood, iron binds to transferrin and is transported in trivalent form to sites of hematopoiesis and to specific depots.
After iron binds to apoferritin, it is deposited in the liver, spleen and bone marrow in the form of ferritin. Iron penetrates the placental barrier and minimal amounts are excreted into breast milk.
Treatment of iron deficiency.
Pharmacotherapeutic group: iron preparation.
ATX code: B03AE10
Pharmacological action
Pharmacodynamics
Iron is the most important microelement in the body. As a coenzyme of cytochrome oxidase, catalase and peroxidase, as well as a component of hemoglobin (Hb), myoglobin and cytochromes, it is involved in many metabolic processes and stimulates erythropoiesis.
The α-amino acid serine included in the drug promotes more efficient absorption of iron and its entry into the systemic circulation, leading to the rapid restoration of its normal content in the body. This ensures better tolerability of the drug and allows you to reduce the required dose of iron.
The daily requirement for iron in adults is 1-2 mg, in pregnant women – 2-5 mg, in children under 7 years old – 0.5-1.5 mg. On average, 10% is absorbed, therefore, to replenish the need for iron, the dose when taken orally should exceed the daily requirement by 10 times.
Pharmacokinetics
After oral administration, about 10-15% of ferrous iron is absorbed in the duodenum and jejunum. Iron absorption is also possible through the mechanism of passive diffusion. Iron absorption increases significantly with iron deficiency and with increased erythropoiesis. In patients with low hemoglobin values and depleted iron stores, absorption may increase to 50-60% and decrease when these indicators normalize. The maximum concentration of iron is achieved 2-4 hours after administration.
In the blood, iron binds to transferrin and is transported in trivalent form to the sites of hematopoiesis and to specific depots.
After iron binds to apoferritin, it is deposited in the liver, spleen and bone marrow in the form of ferritin. Iron crosses the placental barrier and minimal amounts are excreted into breast milk.
When using the drug, persistent darkening of the teeth is possible. Liver or kidney failure increases the risk of iron accumulation. The use of the drug may aggravate ulcerative and inflammatory bowel diseases.
Influence on the ability to drive vehicles and control machines and mechanisms
Not identified.
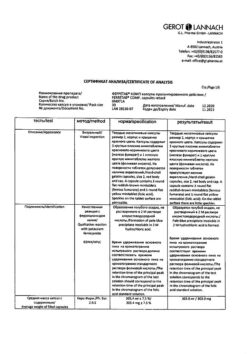
Ferrous sulfate, serine
100 ml contain: active ingredients: iron sulfate heptahydrate 4.720 g, (corresponding to iron II) 0.948 g, D,L-serine 3.560 g; excipients: ascorbic acid 0.8000 g, potassium sorbate 0.1000 g, invert sugar syrup (72.7% TS) 15.1800 g, ethanol (96%) 0.1563 g, cream flavor 0.0125 g, raspberry flavor 0.0500 g, purified water 83.4000 g.
Use during pregnancy and lactation is possible if the potential benefit to the mother outweighs the potential risk to the fetus and child.
– hypersensitivity to the active or auxiliary components of the drug;
– iron absorption disorders (sideroachrestic anemia, lead anemia, thalassemia);
– increased iron content in the body (hemochromatosis, hemolytic anemia);
– anemia not associated with iron deficiency.
With caution
Caution should be exercised when using iron supplements concomitantly with dietary products and supplements containing iron salts (possible risk of overdose).
In patients with inflammation and ulcers of the gastrointestinal mucosa, the balance between the benefits of treatment and the risk of developing exacerbations of gastroenterological diseases during iron therapy should be assessed.
Patients with hereditary fructose or galactose intolerance, lactase deficiency, glucose-galactose malabsorption or sucrose-isomaltose deficiency should not take the drug.
From the immune system: rarely (> 1/10,000 and < 1/1000) allergic skin reactions.
From the gastrointestinal tract: very rarely (< 1/10,000) constipation, diarrhea, abdominal pain, nausea, vomiting.
When taking iron-containing drugs, stool may turn dark (black), which has no clinical significance.
Gastrointestinal disorders can be prevented by gradually increasing the dose at the beginning of treatment or reducing the dose during treatment.
The specific antidote is deferoxamine (desferal).
With simultaneous use of iron salts, the absorption of drugs such as tetracyclines, gyrase inhibitors (for example, ciprofloxacin, levofloxacin, norfloxacin, ofloxacin), penicillamine, levodopa, carbidopa and methyldopa is reduced.
In patients receiving levothyroxine sodium replacement therapy, iron salts reduce its absorption.
Large doses of iron supplements reduce the renal absorption of zinc supplements (the latter are recommended to be taken 2 hours after taking iron supplements).
Iron absorption is reduced by concomitant administration of cholestyramine, antacids (containing aluminum, magnesium, calcium, bismuth) and supplements containing calcium and magnesium.
The simultaneous use of iron salts and non-steroidal anti-inflammatory drugs can enhance the damaging effect of iron on the mucous membrane of the gastrointestinal tract.
In children, when used simultaneously, iron reduces the effectiveness of vitamin E.
Therefore, it is recommended to take all of the above remedies 3-4 hours before or after taking Actiferrin. If it is necessary to prescribe drugs simultaneously, systematic clinical and laboratory monitoring should be carried out.
Tea, coffee, plant foods containing iron chelating agents (such as phosphates, phytates, oxalates), milk, eggs reduce iron absorption.
Ascorbic acid and citric acid increase iron absorption.
Ethanol increases iron absorption and the risk of toxic complications.
Children have a high risk of intoxication with iron preparations; life-threatening conditions can occur when taking 1 g of iron sulfate. Therefore, iron supplements should be stored out of the reach of children.
Symptoms: with accidental ingestion of very large doses of the drug, the following symptoms may be observed: weakness, fatigue, paresthesia, pale skin, cold clammy sweat, decreased blood pressure, palpitations, acrocyanosis, abdominal pain, bloody diarrhea, cyanosis, confusion, weak pulse, hyperthermia, lethargy, seizures, symptoms of hyperventilation, coma.
Signs of peripheral circular collapse appear within 30 minutes after administration; metabolic acidosis, convulsions, fever, leukocytosis, coma – within 12-24 hours; acute renal and hepatic necrosis – after 2-4 days.
Treatment: before specific therapy, measures are taken to remove the drug that has not yet been absorbed from the stomach (gastric lavage), milk and raw eggs are given. Specific therapy is carried out by prescribing deferoxamine (desferal) orally and parenterally. In case of acute poisoning, to bind iron that has not yet been absorbed from the gastrointestinal tract, give 5-10 g of the drug by dissolving the contents of 10-20 ampoules in drinking water.
When poisoning develops, deferoxamine is administered intramuscularly slowly, for children – 15 mg/hour, for adults – 5 mg/kg/hour (up to 80 mg/kg/day); for mild poisoning – children 1 g intramuscularly every 4-6 hours, adults – 50 mg/kg (up to 4 g/day).
In severe cases, accompanied by the development of shock in patients, 1 g of the drug is administered intravenously and symptomatic therapy is carried out. Death mainly occurs due to untimely treatment of patients due to shock.
Hemodialysis is ineffective for removing iron, but can be used to accelerate the removal of the iron-deferoxamine complex, and can also be prescribed for oligo- and anuria. Peritoneal dialysis is also possible.
During a course of treatment with iron supplements, systematic monitoring of serum iron levels and other blood serum parameters is necessary.
Special measures: for severe intoxication – Unithiol (sodium dimercaptopropanesulfonate) parenterally.
Due to the possibility of the formation of neurotoxic complexes, Unithiol should be used with caution.
Store at a temperature not exceeding 25°C.
2 years.
Do not use after expiration date.
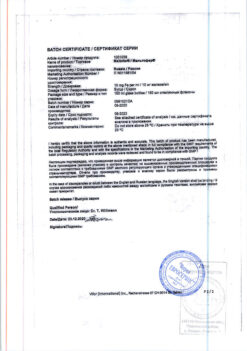
Merkle GmbH, Germany
| Shelf life | 2 years. Do not use after the expiration date. |
|---|---|
| Conditions of storage | Store at a temperature not exceeding 25 ° C. |
| Manufacturer | Merkle GmbH, Germany |
| Medication form | oral drops |
| Brand | Merkle GmbH |

Anemia


Anemia


Buy Aktiferrin®, drops 30 ml with delivery to USA, UK, Europe and over 120 other countries.