-
×
 Lotonel, tablets 5 mg 30 pcs
2 × €9.06
Lotonel, tablets 5 mg 30 pcs
2 × €9.06 -
×
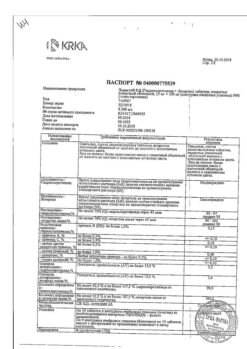
Crestor, 5 mg 28 pcs.
1 × €47.34
-
×
 Klebsiella pneumoniae bacteriophage, 20 ml, 4 pcs.
1 × €30.32
Klebsiella pneumoniae bacteriophage, 20 ml, 4 pcs.
1 × €30.32 -
×
Fosfogliv URSO, 35 mg+250 mg capsules 50 pcs
1 × €23.96
-
×
Glutamic acid, 250 mg 10 pcs
1 × €2.00
-
×
 Sulfasalazine, 500 mg 50 pcs
1 × €8.25
Sulfasalazine, 500 mg 50 pcs
1 × €8.25 -
×
 Rekognan, 100 mg/ml 10 ml 10 pcs
1 × €33.00
Rekognan, 100 mg/ml 10 ml 10 pcs
1 × €33.00 -
×
Lortenza, 10 mg+100 mg 90 pcs
1 × €28.10
-
×
 Singular, 5 mg 14 pcs
1 × €31.41
Singular, 5 mg 14 pcs
1 × €31.41
 Lotonel, tablets 5 mg 30 pcs
Lotonel, tablets 5 mg 30 pcs  Crestor, 5 mg 28 pcs.
Crestor, 5 mg 28 pcs. 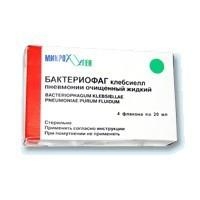 Klebsiella pneumoniae bacteriophage, 20 ml, 4 pcs.
Klebsiella pneumoniae bacteriophage, 20 ml, 4 pcs.  Fosfogliv URSO, 35 mg+250 mg capsules 50 pcs
Fosfogliv URSO, 35 mg+250 mg capsules 50 pcs  Glutamic acid, 250 mg 10 pcs
Glutamic acid, 250 mg 10 pcs 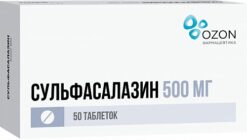 Sulfasalazine, 500 mg 50 pcs
Sulfasalazine, 500 mg 50 pcs  Rekognan, 100 mg/ml 10 ml 10 pcs
Rekognan, 100 mg/ml 10 ml 10 pcs  Lortenza, 10 mg+100 mg 90 pcs
Lortenza, 10 mg+100 mg 90 pcs  Singular, 5 mg 14 pcs
Singular, 5 mg 14 pcs Subtotal: €222.50