No products in the cart.








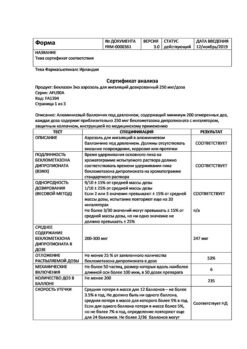
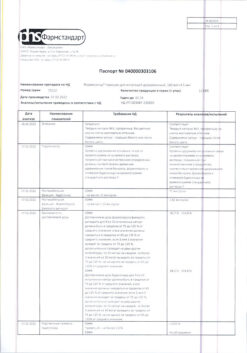
Beclomethasone, aerosol 250 mcg/dose 200 doses
€11.46
Description
Beclomethasone dipropionate is a prodrug and has a weak tropism to GCS-receptors. Under the action of esterases it is converted into the active metabolite – beclomethasone-17-monopropionate (B-17-MP), which has a pronounced local anti-inflammatory effect. It reduces inflammation at the expense of chemotaxis substance formation (influence on “late” allergy reactions), inhibits development of “immediate” allergic reaction (caused by inhibition of arachidonic acid metabolites production and decrease of inflammatory mediators release from mast cells) and improves mucociliary transport.
Beclomethasone decreases the number of mast cells in the bronchial mucosa, it reduces epithelial edema, mucus secretion by bronchial glands, bronchial hyperresponsiveness, margin accumulation of neutrophils, inflammatory exudate and lymphokine production, decreases the macrophages migration, the intensity of infiltration and granulation. It increases the number of active beta-adrenoreceptors, restores the patient’s response to bronchodilators, allows reducing the frequency of their use. It has practically no resorptive effect after inhalation.
It does not arrest bronchospasm, therapeutic effect develops gradually, usually after 5-7 days of course use of beclometasone dipropionate.
Indications
Indications
Baseline therapy of various forms of bronchial asthma in adults and children over 4 years old.
Active ingredient
Active ingredient
Beclomethasone
Composition
Composition
1 dose of the drug contains:
How to take, the dosage
How to take, the dosage
Beclomethasone is for inhaled use only.
Beclomethasone is used regularly (even in the absence of symptoms), and the dose of beclomethasone dipropionate is adjusted for the clinical effect in each case.
In mild bronchial asthma, the inspiratory forced expiratory volume (PEF) or peak expiratory flow (PEF) is greater than 80% of appropriate values, with a PEF variation of less than 20%.
In a moderate course the SPR or PSV is 60-80% of the proper values, the daily variation of PSV is 20-30%.
In a severe course the ROS or PEF is 60 % of the proper values, the diurnal variability of PSV is more than 30 %.
When switching to high-dose inhaled beclomethasone dipropionate, many patients who receive systemic glucocorticosteroids will be able to reduce their dose, to stop them altogether.
The starting dose of Beclomethasone is determined by the severity of bronchial asthma. The daily dose is divided into several doses.
Depending on the patient’s individual response, the dose may be increased until clinical effect occurs or decreased to the lowest effective dose.
Children 4 to 12 years of age
The starting dose is 50 mcg 2 times daily. If necessary, the initial dose can be increased to 100 mcg 2 times a day. The maximum single dose is 200 micrograms.
The maximum daily dose is 400 mcg. The daily dose is divided into 2 to 4 doses.
Adults and children 12 years of age and older:
The recommended starting dose of the drug:
- bronchial asthma of mild course – 200-600 mcg/day;
- bronchial asthma of moderate course – 600-1000 mcg/day;
- bronchial asthma of severe course – 1000-2000 mcg/day.
The treatment of bronchial asthma is based on a step-by-step approach: therapy is started according to the stage corresponding to the severity of the disease. Inhaled GCSs are prescribed in the second step of therapy.
Stage 2. Baseline therapy.
Beclomethasone dipropionate 100-400 mcg 2 times a day.
Stage 3. Baseline therapy.
The use of high-dose inhaled GCS or standard dose, but in combination with long-acting inhaled p-2-adrenomimetics.
Beclomethasone dipropionate in high dose – 800-1600 mcg/day, in some cases megadoses up to 2000 mcg/day.
Stage 4. Severe asthma.
Beclomethasone dipropionate in high dose – 800-1600 mcg/day, in some cases megadoses up to 2000 mcg/day.
Stage 5: Severe asthma.
Beclomethasone dipropionate in high dose (see steps 3 and 4).
Particular patient groups
There is no need to adjust the dose of Beclomethasone in the elderly or in patients with renal or hepatic impairment.
Missing a dose of the drug
If you accidentally miss an inhalation, the next dose should be taken at the correct time according to the treatment regimen.
Patient Instructions for Using an Inhaler
Check the performance of the inhaler before using it for the first time, also if you have not used it for a while, or if it has been cold and then warmed up to room temperature. To check this, remove the protective cap from the inhaler head, turn the can upside down with your index finger on the bottom of the can and your thumb on the top of the inhaler head, shake the can up and down and use your thumb and index finger to push the outlet on the inhaler head to the side. When the aerosol jet appears after the second squeeze, proceed as described below, starting with “Make sure there is no dust or dirt in the outlet tube.
You should do this on a regular basis:
- Remove the protective cap from the inhaler nozzle. Make sure the outlet tube is clean and free from dust and dirt.
- Hold the can upright with your index finger on the bottom of the can and your thumb on the top of the inhaler head. Shake the can up and down.
- Make as deep an exhalation as possible (without tension). Grip the inhaler nozzle outlet tube firmly with your lips. As you inhale, use your thumb and forefinger to release the dose. Continue breathing in slowly.
- Take the inhaler tube out of your mouth and hold your breath for 10 seconds, or as long as you can without straining. Slowly exhale.
- If more than one dose of medicine is needed, wait about a minute and then repeat step 2. Put the protective cap back on the inhaler nozzle.
In steps 3 and 4, take your time. It is important to breathe in as slowly as possible as you release the dose of medicine. Practice in front of a mirror at first. If you notice steam coming out of the corners of your mouth, start again with step 2.
Cleaning the inhaler.
The inhaler head should be cleaned at least once a week. Remove the inhaler nozzle from the cylinder and rinse it and the protective cap with warm water. Do not use hot water. Dry thoroughly, but do not use a heating device for this. Put the protective cap back on the inhaler nozzle and the protective cap back on the balloon. Do not dip the can in water.
Interaction
Interaction
Beclomethasone restores the patient’s response to beta-adrenomimetics, allowing to reduce the frequency of their use.
Co-administration with inducers of microsomal oxidation (including phenobarbital, phenytoin, rifampicin, etc.) may reduce the effectiveness of beclomethasone.
Simultaneous use with methandienone, estrogens, beta2-adrenomimetics, theophylline as well as systemic GCS efficacy of beclomethasone increases.
Simultaneous use of beclomethasone increases the effect of beta-adrenomimetics.
Special Instructions
Special Instructions
Before inhaled medications are administered, the patient should be instructed on how to administer them to ensure that the medication reaches the correct areas of the lungs as completely as possible. The development of oral candidiasis is most likely in patients with high levels of precipitating antibodies against Candida fungus in the blood, indicating a previous fungal infection. Rinse the mouth and throat with water after inhalation. Topical antifungal agents may be used to treat candidiasis while continuing therapy with Beclomethasone.
If patients are taking oral GCS, Beclomethasone is prescribed against a previous dose of GCS, and patients should be in a relatively stable condition. After about 1-2 weeks, the daily dose of oral GCS is gradually reduced. The scheme of dose reduction depends on the duration of previous therapy and the initial dose of GCS. Regular use of inhaled GCS allows in most cases to discontinue oral GCS (patients who need no more than 15 mg of prednisolone may be completely transferred to inhaled therapy). At the same time, in the first months after transfer, the patient’s condition should be closely monitored until the pituitary-adrenal system has recovered sufficiently to ensure an adequate response to stressful situations (e.g., trauma, surgery, or infection).
Allergic reactions (e.g., allergic rhinitis, eczema) that were previously suppressed by systemic drugs may occur when patients are switched from taking systemic GCS to inhaled therapy.
Patients with decreased adrenal cortex function who are transferred to inhaled treatment should have a supply of GCS and should always carry a warning card stating that they need additional systemic GCS administration in stressful situations (after the stressful situation is resolved, the GCS dose can be reduced again). Sudden and progressive worsening of asthma symptoms is a potentially dangerous condition, not infrequently life-threatening, and requires increasing the dose of GCS. An indirect indicator of ineffectiveness of therapy is more frequent use of short-acting 0-2-adrenergic stimulants than before.
Beclomethasone dipropionate for inhalation is not intended for relief of attacks, but for regular daily use. Short-acting (3-2-adreno stimulants (e.g., salbutamol) are used to stop attacks. In severe exacerbation of bronchial asthma or insufficient effectiveness of current therapy should increase the dose of inhaled beclomethasone dipropionate and if necessary, prescribe systemic GCS and antibiotic for infection.
If paradoxical bronchospasm occurs, we should immediately stop using beclomethasone, assess the patient, conduct an examination and if necessary prescribe therapy with other medicines. During long-term use of any inhaled GCS, especially in high doses, systemic effects may be observed (see “Side effects”), but the probability of their development is much lower than when taking GCS orally. Therefore, it is especially important that the dose of inhaled GCS be reduced to the lowest effective dose to control the course of the disease when therapeutic effect is achieved. At a dose of 1500 mcg/day, the drug does not cause significant suppression of adrenal function in most patients. Due to possible adrenal insufficiency special care should be taken and adrenal function indicators should be regularly monitored while transferring patients receiving oral GCS to beclomethasone therapy.
It is recommended to monitor regularly the growth dynamics of children receiving inhaled GCS for a long time.
Injection can be done with special dispensers (spacers) that improve distribution of the drug in the lungs and reduce the risk of side effects.
Abrupt withdrawal of the drug Beklometazon Aerosol is not recommended.
It is necessary to protect the eyes from contact with the drug. Washing after inhalation can prevent skin damage to the eyelids and nose.
The Beclomethasone aerosol can must not be punctured, disassembled, or thrown into a fire, even if it is empty. Like most other aerosol-packed inhalants, Beclomethasone may be less effective at low temperatures. If the cylinder becomes cold, it is recommended that the inhaler nozzle be removed and warmed by hand for several minutes.
Effect on ability to operate vehicles and machinery
No data.
Contraindications
Contraindications
Hypersensitivity to any component of the drug.
Pulmonary tuberculosis.
Pediatric age under 4 years. Beclomethasone containing 250 mcg in 1 dose is not intended for use in pediatrics (i.e., in children under 18 years).
With caution
Side effects
Side effects
Adverse reactions are listed according to the anatomico-physiological classification and occurrence.
Infections: very common – candidiasis of the mouth and pharynx. Use of spacer and rinsing the mouth and throat with water after inhalation reduces the likelihood of these side effects.
Immune system disorders: infrequent – skin hypersensitivity reactions, including rash, urticaria, itching, redness and swelling of the eyes, face, lips and mucosa of the mouth and throat; very rare – angioedema, anaphylactic reactions.
Endocrine system: systemic effects are possible: very rarely – inhibition of adrenal function, growth retardation in children and adolescents, cataract, glaucoma.
Respiratory system: frequently dysphonia (hoarseness of voice) or pharyngeal mucosa irritation, very rarely – paradoxical bronchospasm, which must be treated immediately with inhaled [3-2-adrenergic stimulator of short action. In case of paradoxical bronchospasm it is necessary to immediately stop the use of the drug in inhalation, assess the patient’s condition, conduct the necessary examination and prescribe the necessary treatment.
Skin and subcutaneous fat: often – bruising, thinning of the skin.
Overdose
Overdose
Symptoms:
Acute overdose of the drug may lead to a temporary decrease in adrenal cortical function, which does not require emergency therapy, since the adrenal function recovers within a few days, as evidenced by the plasma concentration of cortisol. In chronic overdose there may be persistent suppression of adrenal cortical function.
Treatment:
In such cases, monitoring of reserve adrenal cortical function is recommended. In case of overdose, treatment with beclomethasone dipropionate may be continued in doses sufficient to maintain the therapeutic effect.
Similarities
Similarities
Beclamethasone Echo easy breathing, Beclamethasone Echo, Beclamethasone-aeronative
Additional information
| Weight | 0.048 kg |
|---|---|
| Shelf life | 3 years. Do not use after the expiration date. |
| Conditions of storage | Store at a temperature not exceeding 25 ° C. |
| Manufacturer | Binnopharm, Russia |
| Medication form | metered aerosol for inhalation |
| Brand | Binnopharm |
Other forms…

Bronchial asthma
€8.71

Bronchial asthma
€9.29

Bronchial asthma
€12.01

Bronchial asthma
€26.59
Related products

Bronchial asthma
€31.41

Medicine
€11.46

Medicine
€5.22

Bronchial asthma
€46.82

Bronchial asthma
€1.75

Bronchial asthma
€4.01

Bronchial asthma
€0.69

€59.30
Buy Beclomethasone, aerosol 250 mcg/dose 200 doses with delivery to USA, UK, Europe and over 120 other countries.
