No products in the cart.

Reddistatin, 20 mg 30 pcs
€1.00
Out of stock
Description
Pharmacotherapeutic group:
Hypolipidemic drug – HMG-CoA reductase inhibitor
CodeATX: C10AA07
Pharmacological properties
Mechanism of action
Rosuvastatin is a selective competitive inhibitor of HMG-CoA reductase, the enzyme that converts Z-hydroxy-3-methylglutaryl coenzyme A to mevalonic acid, a precursor of cholesterol.
Rosuvastatin increases the number of “hepatic” low-density lipoprotein (LDL) receptors on the cell surface, increasing LDL capture and catabolism, which in turn leads to inhibition of very low-density lipoprotein (VLDL) synthesis, thereby reducing total LDL and VLDL.
Pharmacodynamics
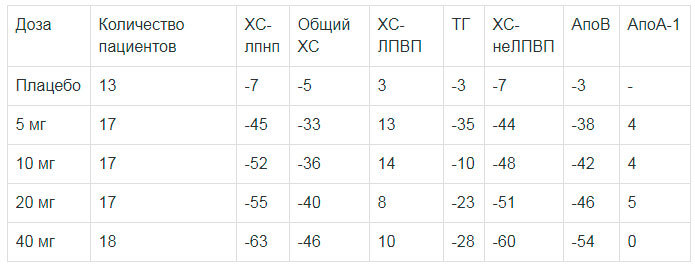
Rosuvastatin reduces elevated LDL cholesterol (XC-LDL), total cholesterol and triglycerides (TG), increases concentrations of high-density lipoprotein cholesterol (HDL-C) and decreases concentrations of apolipoprotein B (ApoB), non-HDL-C, XC-LDL, TG-LDL, and increases apolipoprotein A-I (ApoA-I) concentrations, see Table 1, decreases the ratio of LDL-C/HC-LDL, total CH/LC-LDL and non-LDL-C/HC-LDL and the apoB/ApoA-I ratio.
Therapeutic effect develops within one week after the start of therapy with the drug, after 2 weeks of treatment it reaches 90% of the maximum possible effect.
The maximum therapeutic effect is usually reached by the 4th week of therapy and is maintained with continued regular use of the drug.
Table 1. Dose-dependent effect in patients with primary hypercholesterolemia (type IIa and IIb according to Fredrickson). Mean adjusted percentage change from baseline.
Clinical efficacy
. Rosuvastatin is effective in adult patients with hypercholesterolemia with or without symptoms of hypertriglyceridemia, regardless of their race, sex, or age, including patients with diabetes and familial hypercholesterolemia.
In 80% of patients with hypercholesterolemia of type HA and IB according to Fredrickson (mean baseline concentration of XC-LDL about 4.8 mmol/L) with the use of the drug in dose of 10 mg the concentration of XC-LDL reaches values less than 3 mmol/L.
In patients with heterozygous familial hypercholesterolemia who received rosuvastatin in doses from 20 to 80 mg, positive dynamics of lipid profile parameters were observed (study with 435 patients). After titration to a daily dose of 40 mg (12 weeks of therapy) there is a decrease in LDL-C concentration by 53%. In 33% of patients a LDL-C concentration of less than 3 mmol/l is achieved.
In patients with homozygous familial hypercholesterolemia who took rosuvastatin in doses of 20 and 40 mg, the average decrease in concentration of LDL-C is 22%.
In patients with hypertriglyceridemia with an initial TG concentration of 273 to 817 mg/dL who took rosuvastatin in doses of 5 mg to 40 mg once daily for six weeks, plasma TG concentrations were significantly reduced.
Additive effect is observed in combination with fenofibrate for TG content and with nicotinic acid in lipid-lowering doses for HDL-C content (see also section “Special indications”).
. In patients with low risk of coronary heart disease (CHD) (Framingham Scale risk less than 10% over 10 years), with a mean LDL-C concentration of 4.0 mmol/L (154.5 mg/dL) and subclinical atherosclerosis, as assessed by carotid intima-media complex thickness-TCIM, rosuvastatin at a dose of 40 mg/day significantly slowed the rate of progression of maximum TCIM for 12 carotid segments compared with placebo with a difference of -0.0145 mm/yr (95% confidence interval (CI): -0.0196 to -0.0093; p < 0.001). The dose of 40 mg should only be administered to patients with significant hypercholesterolemia and high risk of cardiovascular disease (CVD).
The results of a study on the use of HMG-CoA reductase inhibitors (statins) for primary prevention showed that rosuvastatin significantly reduced the risk of cardiovascular complications with a relative risk reduction of 44%. Efficacy of therapy was noted after 6 months of using the drug.
There was a statistically significant reduction of 48% in the combined criterion including cardiovascular mortality, stroke and myocardial infarction, a 54% reduction in the occurrence of fatal or non-fatal myocardial infarction, and a 48% reduction in fatal or non-fatal stroke. Overall mortality was reduced by 20% in the rosuvastatin group.
Pharmacokinetics
Absorption and distribution
The maximum plasma concentration of rosuvastatin is reached approximately 5 hours after oral administration. Absolute bioavailability is approximately 20%.
Rosuvastatin is metabolized primarily by the liver, which is the main site of cholesterol synthesis and metabolism of LDL-C. The volume of distribution of rosuvastatin is approximately 134 liters. About 90% of rosuvastatin is bound to plasma proteins, mainly to albumin.
Metabolism
It is subject to limited metabolism (about 10%). Rosuvastatin is a non-core substrate for metabolism by cytochrome P450 isoenzymes.
The main isoenzyme involved in metabolism of rosuvastatin is CYP2C9. CYP2C19, CYP3A4 and CYP2D6 isoenzymes are less involved in metabolism.
The main identified metabolites of rosuvastatin are N-desmethylrosuvastatin and lactone metabolites. N-desmethylrosuvastatin is about 50% less active than rosuvastatin, lactone metabolites are pharmacologically inactive. More than 90% of the pharmacological activity for inhibition of circulating HMG-CoA reductase is provided by rosuvastatin, the rest by its metabolites.
Elimation
About 90% of the dose of rosuvastatin is excreted unchanged through the intestine (including absorbed and unabsorbed rosuvastatin). The remainder is excreted by the kidneys. Plasma elimination half-life (T1/2) is approximately 19 hours. The elimination half-life does not change with increasing drug dose. Mean geometric plasma clearance is approximately 50 L/hour (coefficient of variation 21.7%).
As with other HMG-CoA reductase inhibitors, the membrane cholesterol transporter is involved in the “hepatic” uptake of rosuvastatin and has an important role in hepatic elimination of rosuvastatin.
Linearity
The systemic exposure of rosuvastatin increases in proportion to the dose. Pharmacokinetic parameters do not change with daily administration.
Particular patient populations. Age and sex
Pass and age have no clinically significant effect on the pharmacokinetics of rosuvastatin.
Ethnic groups
. Pharmacokinetic studies have shown an approximately two-fold increase in the median area under the pharmacokinetic concentration-time curve (AUC) and maximum plasma concentration (TAC) of rosuvastatin in patients of the Mongoloid race (Japanese, Chinese, Filipino, Vietnamese, and Korean) compared with Caucasians; Hindus showed a 1.3-fold increase in median AUC and Cmax.
Pharmacokinetic analysis showed no clinically significant differences in pharmacokinetics among Caucasoid and non-Hispanic races.
Renal failure
In patients with mild to moderately severe renal failure the plasma concentration of rosuvastatin or N-desmethylrosuvastatin does not change significantly. In patients with severe renal insufficiency (creatinine clearance (CK) less than 30 ml/min) the plasma concentration of rosuvastatin is 3 times higher, and N-desmethylrosuvastatin concentration is 9 times higher than in healthy volunteers. Plasma concentrations of rosuvastatin were approximately 50% higher in patients on hemodialysis than in healthy volunteers.
Hepatic failure
In patients with various stages of hepatic failure no increase in the elimination half-life of rosuvastatin was found (in patients with a Child-Pugh score of 7 or lower). Two patients with Child-Pugh scores 8 and 9 showed at least 2-fold increase in half-life. There is no experience with rosuvastatin in patients with more than a Child-Pugh score of 9.
Genetic polymorphism
. HMG-CoA reductase inhibitors, including rosuvastatin, bind to the transport proteins OATP1B1 (organic anion transport polypeptide involved in statin uptake by hepatocytes) and BCRP (efflux transporter). Carriers of SLC01B1 (OATP1B1) C.521CC and ABCG2 (BCRP) C.421AAA genotypes had 1.6 and 2.4-fold increased exposure (AUC) to rosuvastatin, respectively, compared with carriers of SLC01B1 C.521TT ABCG2 C.421CC genotypes.
Indications
Indications
Active ingredient
Active ingredient
Composition
Composition
How to take, the dosage
How to take, the dosage
Ingestion. Any time of the day, regardless of meals. The tablet should not be chewed or crushed and should be swallowed whole with water.
Before therapy, the patient should start a standard hypocholesterolemic diet and continue it during the whole period of treatment.
The dose of the drug should be adjusted individually depending on the goals of therapy and the therapeutic response to treatment, taking into account current accepted recommendations for target lipid concentrations.
The recommended starting dose for patients starting rosuvastatin or for patients transferred from other HMG-CoA reductase inhibitors should be 5 or 10 mg of the drug once daily. When choosing the initial dose, the individual cholesterol content should be guided and the possible risk of cardiovascular complications should be taken into account, as well as the potential risk of side effects should be assessed. If necessary, the dose may be increased in 4 weeks (see section “Pharmacodynamics”).
With regard to the possible development of side effects when taking a dose of 40 mg compared to lower doses of the drug (see section “Side Effects”). Due to the possible development of side effects of 40 mg compared to lower doses of the drug (see “Side Effects”), increasing the dose to 40 mg, after an additional dose above the recommended initial dose for 4 weeks of therapy, may only be undertaken in patients with severe hypercholesterolemia and with a high risk of cardiovascular complications (especially in patients with familial hypercholesterolemia), in whom the desired result of therapy was not achieved at the 20 mg dose and will be under medical supervision (see “Special Considerations”). We recommend especially close monitoring of patients receiving 40 mg.
Prescribing a dose of 40 mg to patients who have not previously seen a physician is not recommended. After 2-4 weeks of therapy and/or when increasing the dose of the drug, lipid metabolism parameters should be monitored, and the dose should be adjusted if necessary.
Elderly patients
Dose adjustment is not required.
Patients with renal impairment
Dose adjustment is not necessary in patients with mild to moderate renal impairment. In patients with severe renal failure (CKD less than 30 ml/min) the drug is contraindicated. The drug administration in dose 40 mg is contraindicated in patients with moderate renal impairment with CKD 30-60 ml/min (see section “Special indications” and “Pharmacodynamics”). In patients with moderate renal dysfunction, a starting dose of 5 mg is recommended.
Patients with hepatic impairment
The drug is contraindicated in patients with active liver disease (see section “Contraindications”).
Special populations. Ethnic groups
When studying pharmacokinetic parameters of rosuvastatin in patients belonging to different ethnic groups, an increased systemic concentration of rosuvastatin was noted among Japanese and Chinese (see section “Special indications”).
This fact should be considered when prescribing the drug in this group of patients. When prescribing doses of 10 mg and 20 mg, the recommended starting dose of the drug for mongoloid patients is 5 mg. A dose of 40 mg is contraindicated in patients of mongoloid race (see Contraindications).
Genetic polymorphisms
Carriers of the SLCOIBI (OATP1B1) C.521CC and ABCG2 (BCRP) C.421AA there was an increased exposure (AUC) to rosuvastatin compared with SLCOIBI C.521T ABCG2 C.421CC genotype carriers. For C.521CC or C.421AA genotype carriers the recommended maximum dose of rosuvastatin is 20 mg once daily (see sections “Pharmacokinetics”, “Special Considerations” and “Interaction with Other Medicinal Products and Other Drug Interactions”).
Patients with predisposition to myopathy
The drug is contraindicated at a dose of 40 mg in patients with factors that may indicate a predisposition to myopathy (see Contraindications). When doses of 10 mg and 20 mg are prescribed, the recommended starting dose for this group of patients is 5 mg (see Contraindications).
Companion therapy
Rosuvastatin binds to various transport proteins (in particular to OATP1B1 and BCRP). When co-administering rosuvastatin with drugs (such as cyclosporine, some HIV protease inhibitors, including the combination of ritonavir with atazanavir, lopinavir and/or tipranavir) that increase the plasma concentration of rosuvastatin through interaction with transport proteins, the risk of myopathy including rhabdomyolysis may increase (see sections “Cautions” and “Interaction with other medicinal products and other drug interactions”).
The instructions for use of these drugs should be read before prescribing them together with rosuvastatin. In such cases, the possibility of prescribing alternative therapy or temporary discontinuation of rosuvastatin should be assessed. If co-administration is necessary, the benefit-risk ratio of concomitant therapy with rosuvastatin should be assessed and the possibility of reducing its dose should be considered (see section “Interaction with other medicinal products and other drug interactions”).
Interaction
Interaction
Influence of the use of other drugs on rosuvastatin
Transport protein inhibitors
10 mg once daily, 10 days
7.1-fold increase
10 mg once
Increased 3.1-fold
Simeprevir 150 mg once daily, 7 days
10 mg once
/p>
2.8-fold increase
Lopinavir 400 mg / ritonavir 100 mg, 2 times daily, 17 days
20 mg once daily, 7 days
2.1-fold increase
Clopidogrel 300 mg (loading dose) followed by 75 mg 24 hours later
20 mg once
2x increase
Hemfibrozil 600 mg 2 times daily, 7 days
80 mg once
1.9-fold increase
Eltrombopag 75 mg once daily, 10 days
10 mg once
1.6-fold increase
10 mg once daily, 7 days
Increased 1.5-fold
Tipranavir 500 g / ritonavir 200 mg, 2 times daily, 11 days
10 mg once
1.4-fold increase
Dronedarone 400 mg 2 times daily
No data
1.4-fold increase
Itraconazole 200 mg once daily, 5 days
10 or 80 mg once
1.4-fold increase
Ezetimibe 10 mg once daily, 14 days
10 mg once daily, 14 days
1.2-fold increase
Fosamprenavir 700 mg / ritonavir, 100 mg, 2 times daily, 8 days
10 mg once
No change
Aleglitazar 0.3 mg, 7 days
40 mg, 7 days
No change
Silymarin 140 mg 3 times daily, 5 days
10 mg once
No change
Phenofibrate 67 mg 3 times daily, 7 days
/td>
10 mg, 7 days
No change
Rifampin 450 mg once daily, 7 days
20 mg once
No change
Ketoconazole 200 mg 2 times daily, 7 days
80 mg once
No change
Fluconazole 200 mg once daily, 11 days
80 mg once
No change
/p>
Erythromycin 500 mg 4 times daily, 7 days
/p>
80 mg once
28% reduction
20 mg once
47% reduction
/td>
The effect of rosuvastatin use on other drugs
Special Instructions
Special Instructions
Renal effects
In patients receiving high doses of rosuvastatin (mainly 40 mg), tubular proteinuria was observed, which in most cases was transient. Such proteinuria was not indicative of acute kidney disease or progression of renal disease. The incidence of serious renal dysfunction is increased when taking 40 mg of rosuvastatin. In patients taking the drug at a dose of 40 mg, it is recommended to monitor renal function parameters.
Musculoskeletal disorders
Myalgia, myopathy and, rarely, rhabdomyolysis have been observed with rosuvastatin at all doses, and especially with doses above 20 mg.
Creatine phosphokinase (CPK) determination
The determination of CPK activity should not be performed after vigorous exercise or in the presence of other possible causes of increased CPK activity, which may lead to misinterpretation of results. If the baseline CPK level is significantly elevated (more than 5 times the upper limit of normal), the measurement should be repeated after 5-7 days. Therapy should not be started if the repeat measurement confirms the baseline CPK level (5 times higher than the upper limit of normal).
Pending therapy
When prescribing rosuvastatin, as well as other HMG-CoA reductase inhibitors, caution should be exercised in patients with existing risk factors for myopathy/rhabdomyolysis (see section “Caution”), the risk/benefit ratio of therapy should be considered and clinical monitoring should be performed.
In therapy
The patient should be informed of the need to promptly inform the physician if muscle pain, muscle weakness, or cramps occur unexpectedly, especially if combined with malaise or fever. In such patients, monitoring of CPK activity should always be performed. Treatment should be discontinued if CPK levels are more than 5 times the upper limit of normal or if muscle symptoms are severe and cause daily discomfort, even if CPK activity is not more than 5 times the upper limit of normal.
If symptoms disappear and CPK activity returns to normal, re-prescribing rosuvastatin or other HMG-CoA reductase inhibitors at lower doses with close monitoring of the patient should be considered. Routine monitoring of CPK activity in the absence of symptoms is unnecessary.
There have been very rare cases of immune-mediated necrotizing myopathy with clinical manifestations as persistent proximal muscle weakness and increased serum CPK activity during treatment or upon discontinuation of statins, including rosuvastatin. Additional muscular and nervous system studies, serological studies, and therapy with immunosuppressive agents may be required. No evidence of increased skeletal muscle effects with rosuvastatin and concomitant therapy has been noted.
Contraindications
Contraindications
For daily doses of 5 mg, 10 mg and 20 mg:
– hypersensitivity to rosuvastatin or any of the components of the drug;
– Lactose intolerance, lactase deficiency or glucose-galactose malabsorption (because the drug contains lactose);
– Age less than 18 years (efficacy and safety not established);
– active liver disease, including a persistent increase in “hepatic” transaminase activity and any increase in “hepatic” transaminase activity in serum more than 3 times the upper limit of normal;
– severe renal dysfunction (CKG less than 30 ml/min);
– myopathy;
– concomitant administration of cyclosporine;
– in women: pregnancy, breastfeeding period, lack of reliable methods of contraception;
– patients predisposed to the development of myotoxic complications.
For a daily dose of 40 mg:
– hypersensitivity to rosuvastatin or any of the components of the drug;
– active hepatic disease, including a persistent increase in hepatic transaminase activity and any increase in serum hepatic transaminase activity greater than 3 times the upper limit of normal;
– presence of risk factors for myopathy/rhabdomyolysis (moderate renal failure (CKD less than 60 ml/min), hypothyroidism, myopathy in anamnesis (including hereditary forms), myotoxicity with a history of taking other HMG-CoA reductase inhibitors or fibrates, excessive alcohol intake, conditions that may lead to increased plasma concentrations of rosuvastatin, concomitant use of fibrates, use in patients of mongoloid race);
– concomitant use of cyclosporine;
– in women: pregnancy, breastfeeding period, lack of reliable methods of contraception;
– use in patients predisposed to the development of myotoxic complications;
– Lactose intolerance, lactase deficiency or glucose-galactose malabsorption (the drug contains lactose);
– Under 18 years of age (efficacy and safety not established);
Cautions
For a daily dose of 5 mg. 10 mg and 20 mg
Having a risk of myopathy/rhabdomyolysis – renal failure, hypothyroidism; personal or family history of hereditary muscle disease and prior history of muscle toxicity with other HMG-CoA reductase inhibitors (statins) or fibrates; excessive alcohol consumption; conditions with increased plasma concentrations of rosuvastatin; age over 65 years; history of liver disease; sepsis; arterial hypotension; major surgical interventions; trauma; severe metabolic, endocrine or electrolyte disorders; uncontrolled seizures; race (mongoloid race); concomitant use of fibrates.
For a daily dose of 40 mg
Having a risk of myopathy/rhabdomyolysis – mild renal failure (CK more than 60 ml/min); age over 65 years; history of liver disease; sepsis; arterial hypotension; major surgical interventions; trauma; severe metabolic, endocrine, or electrolyte disorders; uncontrolled epilepsy.
Pediatric use
The efficacy and safety of the drug in children under 18 years of age has not been established. The experience of using the drug in pediatric practice is limited to a small number of children (8 years and older) with familial homozygous hypercholesterolemia. Currently, it is not recommended to use rosuvastatin in children under 18 years of age.
Side effects
Side effects
The side effects observed with rosuvastatin are usually mild and go away on their own. As with other HMG-CoA reductase inhibitors, the incidence of side effects is mostly dose-dependent,
Frequency of adverse effects is as follows: frequent (1/10 to 1/100 appointments); infrequent (1/100 to 1/1000 appointments); rare (1/1000 to 1/10 000 appointments), very rare (< 1/10 000); frequency unknown (cannot be calculated from available data).
Disorders of the blood and lymphatic system
Rarely, thrombocytopenia.
Nervous system disorders
Often – headache, dizziness; very rare – peripheral neuropathy, loss or reduction of memory; frequency unknown – sleep disturbance, including insomnia and “nightmares” dreams.
Mental disorders
Prevalence unknown – depression.
Disorders of the digestive system
Often – constipation, nausea, abdominal pain; infrequently – vomiting; rarely – pancreatitis; frequency unknown – diarrhea.
Hepatic and biliary tract disorders
Rarely – transient increase in “hepatic” transaminase activity in a small number of patients; very rare – hepatitis, jaundice.
Respiratory system disorders
Infrequent unknown – cough, shortness of breath.
Disorders of the immune system
Rarely – hypersensitivity reactions, including angioedema. Endocrine system disorders Often – type 2 diabetes mellitus.
Musculoskeletal and connective tissue disorders
Often – myalgia; rarely – myopathy (including myositis), rhabdomyolysis (in patients treated with doses of > 20 mg per day); very rare – arthralgia, tendopathies, possibly with tendon rupture; frequency unknown – immune-mediated necrotizing myopathy.
Skin and subcutaneous tissue disorders
Infrequent – skin itching, skin rash, urticaria; frequency unknown – Stephen-Johnson syndrome.
Recreational and urinary tract disorders
Often – proteinuria (with an incidence greater than 3% in patients receiving a dose of 40 mg), decreasing with therapy and not associated with the occurrence of renal disease, urinary tract infection; very rare – hematuria.
Gender and breast disorders
Very rare – gynecomastia.
Influence on the indicators of laboratory and instrumental studies
Infrequent – transient dose-dependent increase in serum creatine phosphokinase-CFC activity (if increased by more than 5 times the upper limit of normal, therapy should be temporarily suspended), increased plasma concentration of glycosylated hemoglobin; frequency unknown – thyroid function abnormality, increased concentration of glucose, bilirubin, alkaline phosphatase activity, gamma-glutamyl transpeptidase.
Others
Often – asthenia; frequency unknown – peripheral edema.
Some statins
The following side effects have been reported with some statins: erectile dysfunction; isolated cases of interstitial lung disease, especially with long-term use; type 2 diabetes: frequency depends on the presence or absence of risk factors (fasting blood glucose concentration 5.6 – 6.9 mmol/l, body mass index (BMI) >30 kg/m2, hypertriglyceridemia, arterial hypertension in the history.
Overdose
Overdose
Similarities
Similarities
Additional information
| Shelf life | 3 years. Do not use after the expiration date stated on the package. |
|---|---|
| Conditions of storage | At the temperature not more than 25 ° C. Keep out of reach of children! |
| Manufacturer | Dr. Reddy's, India |
| Medication form | pills |
| Brand | Dr. Reddy's |
Related products

Asthenia, weakness
€11.27


Asthenia, weakness
€14.86

Medicine
€4.04

Asthenia, weakness
€29.25

Asthenia, weakness
€5.76

Asthenia, weakness
€13.09

€13.99


Asthenia, weakness
€15.17
Buy Reddistatin, 20 mg 30 pcs with delivery to USA, UK, Europe and over 120 other countries.
