-
×
 Amoxiclav Quicktab, 500 mg+125 mg 14 pcs
1 × €9.54
Amoxiclav Quicktab, 500 mg+125 mg 14 pcs
1 × €9.54 -
×
 Primadophilus for children, powder, 141.75 g
1 × €29.24
Primadophilus for children, powder, 141.75 g
1 × €29.24 -
×
 Rekognan, 100 mg/ml 10 ml 10 pcs
1 × €33.00
Rekognan, 100 mg/ml 10 ml 10 pcs
1 × €33.00 -
×
Veroshpilactone, 50 mg capsules 30 pcs
1 × €5.14
-
×
 Metronidazole, tablets 250 mg 40 pcs
1 × €3.96
Metronidazole, tablets 250 mg 40 pcs
1 × €3.96 -
×
Leovit Kisel General Strengthening 20 g, 5 pcs.
1 × €5.82
-
×
Elcar, 300 mg/ml 100 ml
1 × €19.26
-
×
Moxonidine-SZ, 0.4 mg 28 pcs
1 × €7.13
-
×
Ascorbic acid powder with lemon flavor 500 mg sachets, 30 pcs.
1 × €4.77
-
×
Moxonidine-SZ, 0.2 mg 28 pcs.
1 × €4.36
 Amoxiclav Quicktab, 500 mg+125 mg 14 pcs
Amoxiclav Quicktab, 500 mg+125 mg 14 pcs  Primadophilus for children, powder, 141.75 g
Primadophilus for children, powder, 141.75 g  Rekognan, 100 mg/ml 10 ml 10 pcs
Rekognan, 100 mg/ml 10 ml 10 pcs  Veroshpilactone, 50 mg capsules 30 pcs
Veroshpilactone, 50 mg capsules 30 pcs 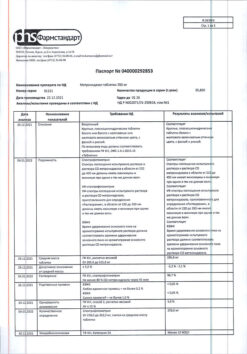 Metronidazole, tablets 250 mg 40 pcs
Metronidazole, tablets 250 mg 40 pcs  Leovit Kisel General Strengthening 20 g, 5 pcs.
Leovit Kisel General Strengthening 20 g, 5 pcs.  Elcar, 300 mg/ml 100 ml
Elcar, 300 mg/ml 100 ml  Moxonidine-SZ, 0.4 mg 28 pcs
Moxonidine-SZ, 0.4 mg 28 pcs  Ascorbic acid powder with lemon flavor 500 mg sachets, 30 pcs.
Ascorbic acid powder with lemon flavor 500 mg sachets, 30 pcs.  Moxonidine-SZ, 0.2 mg 28 pcs.
Moxonidine-SZ, 0.2 mg 28 pcs. Subtotal: €122.22














