-
×
 Gentos, drops 50 ml
1 × €21.20
Gentos, drops 50 ml
1 × €21.20 -
×
Atheroklefit, drops, 100 ml
1 × €9.55
-
×
Desrinit, spray 50 mcg/dose 18 g 140 doses
1 × €14.51
-
×
Atheroklefit Bio, capsules, 30 pcs.
1 × €11.10
-
×
 Budenofalk, 3 mg capsules 20 pcs
1 × €31.65
Budenofalk, 3 mg capsules 20 pcs
1 × €31.65 -
×
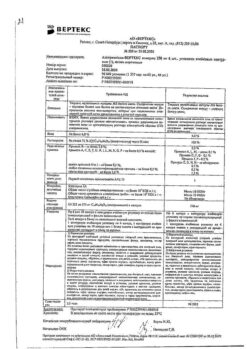
Perindopril PLUS, tablets 2.5mg+8 mg 30 pcs
1 × €10.21
-
×
 Tavanic, 500 mg 10 pcs
1 × €15.01
Tavanic, 500 mg 10 pcs
1 × €15.01 -
×
Lotonel, tablets 5 mg 60 pcs
1 × €14.32
-
×
Formidron, 100 ml
1 × €2.22
-
×
Betoptik, eye drops 0.5% 5 ml
1 × €12.76
 Gentos, drops 50 ml
Gentos, drops 50 ml  Atheroklefit, drops, 100 ml
Atheroklefit, drops, 100 ml  Desrinit, spray 50 mcg/dose 18 g 140 doses
Desrinit, spray 50 mcg/dose 18 g 140 doses  Atheroklefit Bio, capsules, 30 pcs.
Atheroklefit Bio, capsules, 30 pcs.  Budenofalk, 3 mg capsules 20 pcs
Budenofalk, 3 mg capsules 20 pcs  Perindopril PLUS, tablets 2.5mg+8 mg 30 pcs
Perindopril PLUS, tablets 2.5mg+8 mg 30 pcs  Tavanic, 500 mg 10 pcs
Tavanic, 500 mg 10 pcs  Lotonel, tablets 5 mg 60 pcs
Lotonel, tablets 5 mg 60 pcs  Formidron, 100 ml
Formidron, 100 ml  Betoptik, eye drops 0.5% 5 ml
Betoptik, eye drops 0.5% 5 ml Subtotal: €142.53