No products in the cart.

Atorvastatin Alkaloid, 10 mg 30 pcs
€1.00
Out of stock
Description
Pharmacodynamics
Atorvastatin is a selective competitive inhibitor of HMG-CoA reductase – the enzyme that determines the limiting rate of cholesterol biosynthesis, responsible for converting 3-hydroxy-3 -methylglutaryl coenzyme A into mevalonate, a precursor of sterols, including cholesterol. In the liver, triglycerides and cholesterol are incorporated into very low density lipoproteins (VLDL), entering the blood plasma and being transported to peripheral tissues. From VLDL form low-density lipoproteins (LDL), which are catabolized mainly through interaction with high-affinity LDL receptors.
Atorvastatin reduces plasma levels of cholesterol and lipoproteins by inhibiting HMG-CoA reductase and cholesterol synthesis in the liver, as well as by increasing the number of “hepatic” LDL receptors on the cell surface, increasing capture and catabolism of LDL.
Atorvastatin reduces LDL production and the number of LDL particles. Atorvastatin causes pronounced and sustained increase in LDL receptor activity combined with favorable changes in the quality of circulating LDL particles.
Dose-dependently reduces LDL levels in patients with homozygous hereditary hypercholesterolemia, resistant to therapy with other hypolipidemic agents.
Dose/effect studies have shown that atorvastatin reduces total cholesterol (by 30-46%), LDL cholesterol (by 41-61%), apolipoprotein B (by 34-50%) and triglycerides (by 14-33%), while causing an increase, to varying degrees, in HDL cholesterol and apolipoprotein A levels. These results were similar in patients with heterozygous familial hypercholesterolemia, nonfamilial forms of hypercholesterolemia and mixed hyperlipidemia, including patients with insulin-independent diabetes.
Due to decreased levels of total cholesterol, LDL cholesterol and apolipoprotein B the risk of cardiovascular disease and, consequently, the risk of death decreases. Studies of the effect of atorvastatin on cardiovascular morbidity and mortality have not yet been completed.
No differences in safety, efficacy or achievement of hypolipidemic therapy goals were noted when using the drug in elderly patients compared to the general population.
Pharmacokinetics
Absorption
After oral administration atorvastatin is rapidly absorbed into the blood. Maximal concentration (Сmax) in plasma is reached within 1-2 hours, Сmax in women is 20% higher, area on curve “concentration-time” (AUC) – 10% lower; Сmax in patients with alcoholic liver cirrhosis is 16 times higher, AUC – 15 times higher. Food intake slightly reduces speed and duration of drug absorption (by 25% and 9% respectively), but cholesterol decrease is similar to that of atorvastatin without food. Absolute bioavailability of atorvastatin is approximately 12%, systemic bioavailability, which determines inhibitory activity against HMG-CoA reductase – 30%. Low systemic bioavailability is due to presystemic metabolism in the mucosa of gastrointestinal tract and during “first passage” through the liver.
Distribution
Average volume of distribution of atorvastatin is approximately 381 l. It is metabolized mainly in liver with participation of CYP3A4, CYP3A5 and CYP3A7 cytochrome Р450 isoenzymes with formation of pharmacological active metabolites (ortho- and parahydroxylated derivatives, beta-oxidation products). In vitro, ortho- and parahydroxylated metabolites have an inhibitory effect on HMG-CoA reductase, comparable with that of atorvastatin. The inhibitory effect of the drug against HMG-CoA reductase is approximately 70% determined by the activity of circulating metabolites.
Excretion
Atorvastatin is excreted mainly with bile after hepatic and/or extrahepatic metabolism (is not subject to marked hepatic recirculation).
The elimination half-life is 14 hours. Inhibitory activity against HMG-CoA reductase lasts for about 20-30 hours due to the presence of active metabolites. Less than 2% of the oral dose is detected in the urine. It is not excreted during hemodialysis.
Indications
Indications
Active ingredient
Active ingredient
Composition
Composition
How to take, the dosage
How to take, the dosage
Interaction
Interaction
Special Instructions
Special Instructions
Contraindications
Contraindications
With caution: alcohol abuse, history of liver disease, severe electrolyte balance disorders, endocrine and metabolic disorders, arterial hypotension, severe acute infections (sepsis), uncontrolled epilepsy, extensive surgery, trauma, skeletal muscle diseases.
Side effects
Side effects
Overdose
Overdose
Pregnancy use
Pregnancy use
Similarities
Similarities
Additional information
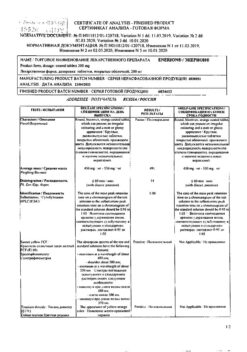
| Shelf life | 2 years. |
|---|---|
| Conditions of storage | At the temperature not more than 30 ° C. Keep out of reach of children. |
| Manufacturer | Alkaloid AD Skopje, Republic of Northern Macedonia |
| Medication form | pills |
| Brand | Alkaloid AD Skopje |
Other forms…

Atherosclerosis
€25.01

Atherosclerosis
€9.98

Atherosclerosis
€11.05

Atherosclerosis
€9.27

Atherosclerosis
€9.11


Atherosclerosis
€31.29
Related products

Asthenia, weakness
€29.25


Asthenia, weakness
€19.26

Asthenia, weakness
€5.76


Asthenia, weakness
€9.21

Asthenia, weakness
€13.09


Asthenia, weakness
€14.86


Asthenia, weakness
€15.17


Asthenia, weakness
€3.23
Buy Atorvastatin Alkaloid, 10 mg 30 pcs with delivery to USA, UK, Europe and over 120 other countries.
